马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?注册
×
中文版:腹腔镜治疗泌尿生殖道脱垂(中文图文演示)
LAPAROSCOPIC TREATMENT OF GENITOURINARY PROLAPSE
Authors
JL Hoepffner, R Gaston
Abstract
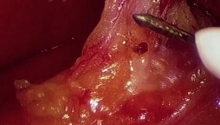
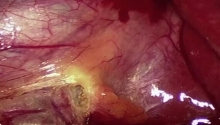
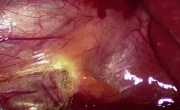
The description of the laparoscopic treatment of genitourinary prolapse covers all aspects of the surgical procedure used for the management of genital prolapse.
Operating room set up, position of patient and equipment, instruments used are thoroughly described. The technical key steps of the surgical procedure are presented in a step by step way: exposure, dissection, posterior prosthesis, closure, promontory, vesico-vaginal dissection, anterior mesh, promontory fixation, repair of peritoneum, drainage/closure.
Consequently, this operating technique is well standardized for the management of this condition. |
|

 腹腔镜胆囊切除术中胆囊动脉出血的处理
腹腔镜胆囊切除术中胆囊动脉出血的处理
 MAGPI 尿道下裂修复
MAGPI 尿道下裂修复
 腹腔镜胆囊切除术
腹腔镜胆囊切除术
 坏疽性胆囊 - 腹腔镜胆囊切除术及技巧
坏疽性胆囊 - 腹腔镜胆囊切除术及技巧

 发表于 2016-7-21 10:31:21
发表于 2016-7-21 10:31:21
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主