10. Approach/hepatic pedicle
Cholecystectomy is performed first in order to expose the superior portion of the right portal pedicle.
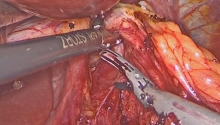
The triangle of Calot is exposed by retracting Hartmann’s pouch caudad and to the right. The anterior and posterior peritoneal leaves are divided down to the inferior surface of the liver. The cystic duct and the cystic artery are identified and separated. The cystic artery is divided first, after ligation or cauterization of the gallbladder neck. The cystic duct is subsequently divided.
With the left hand, the first assistant pulls down the first duodenum to expose the anterior surface of the hepatoduodenal ligament. Segment 4 is lifted cephalad with a valve placed on its lower surface. This exposes the hilar plate, which is the reflection of the peritoneum of the porta hepatis on the capsule of segment 4, where the visceral peritoneum is slightly thickened.
• Hilar plate
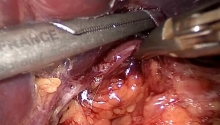
The peritoneum is opened at the level of the hilar plate parallel to the edge of segment 4, starting with the right part of the hilum. Only this right part should be divided.
It is best to use bipolar cauterization before dividing the peritoneum with sharp scissors.
The decapsulated liver parenchyma appears at the upper part of the peritoneal incision. It is retracted slightly cephalad. The confluence of the right and left hepatic ducts is identified at the lower part of the incision, as well as the distal end of the right hepatic duct. This pulls the liver parenchyma off the right hepatic pedicle, which is lengthened artificially by this maneuver. The dissection of the right hepatic duct should be interrupted at this point.
• Right branch of the portal vein
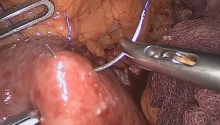
The peritoneum on the right inferior border of the porta hepatis is opened longitudinally, where the portal vein lies superficially. In order to facilitate the exposure, the first assistant slightly rotates the inferior part of the porta hepatis clockwise with the left hand. The portal vein lies just below the peritoneal layer.
The anterior and posterior surfaces of the portal vein are dissected free. The portal vein receives no tributaries in this segment.
The peritoneal incision is then extended cephalad along the right edge of the right portal vein. The superficial part of the hepatic pedicle is gently retracted cephalad with a small retractor. The dissection of the anterior surface of the portal vein and the exposure of the origin of the left portal vein is facilitated by a slight traction on the left portal vein. The areolar tissue situated between the main portal branches is cautiously retracted with the tip of blunt scissors to expose the origin of the right portal vein.
A tape can then be placed around the right portal vein. The dissecting instrument should be used with extreme caution around the right portal vein to avoid potential injury to the portal bifurcation or to the origin of the left portal vein.
If the right portal vein is not sufficiently freed, the portal bifurcation may be injured during the passage of the dissector, potentially resulting in massive bleeding.
The repair of this injury is very difficult. It is best to clamp the portal vein to decrease the blood flow.
A small branch supplying the right part of segment 1 originates from the right or posterior surface of the right portal branch near the portal bifurcation. This branch can be accidentally injured during isolation of the right portal vein. It is therefore preferable to ligate and divide it before taping.
The most common anatomical variations are either the division of the portal trunk into three branches or a segmental right portal vein arising from the left portal vein. If there are two different portal branches coursing towards the right liver, tape should be placed around them.
• Hepatic artery
The right hepatic artery is searched for in the lymphatic tissue anterior to the right portal branch. This localisation is constant, even in cases of an anomalous pattern of the arterial tree (early division of the right hepatic artery, for example).
The lymphatic tissue is cautiously opened after performing bipolar cauterization. The right hepatic artery might already be divided into segmental or subsegmental branches. All of the remaining lymphatic tissue surrounding the artery is divided and the artery and its branches (if present) are placed on tape. |

 腹腔镜治疗正中弓状韧带综合征(MALS)——
腹腔镜治疗正中弓状韧带综合征(MALS)——
 腹腔镜治疗药物治疗失败后早期小肠梗阻复发
腹腔镜治疗药物治疗失败后早期小肠梗阻复发
 腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
 腹腔镜下全结肠切除术联合末端回肠造口术治
腹腔镜下全结肠切除术联合末端回肠造口术治

 楼主
楼主














 显身卡
显身卡