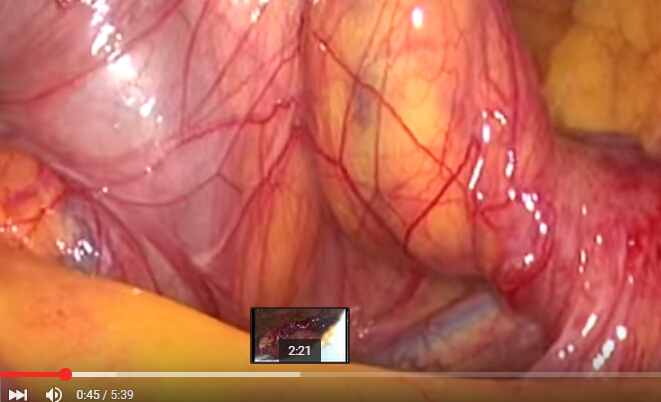
An 43-year-old man who was suffering from a intermittent mesogastric and ipogastric pain was admitted to the hospital for further examination.
The results of laboratory tests performed upon admission were normal. CT Scan revealed an encapsulated circumscribed cluster of jejunal loops in the left upper quadrant. The proximal side of the cluster was shown to be the jejunum near the ligament of Treitz, and the hernia orifice was adjacent to the left side of the superior mesenteric artery and vein. The endovenous contrast medium showed the so- called perfusion cut-off sign that define a midgut volvolus. No dilatation of the jejunum was observed. These radiologic findings suggested an internal hernia of some kind and a paraduodenal hernia with volvulus was the most likely.
Emergent laparoscopic surgery was performed to treat the internal hernia. Three ports were placed on the abdominal wall (right lumbar region, right hypochondriac and right iliac fossa).
During laparoscopy the small bowel was found completely herniated under the mesenteric vessel. After the adhesiotomy, the jejunum entrapped in the hernia was gradually reduced and examinated.
There was nor apparent abnormality of the transverse or descending colon nor visible hernia sac Then the hernia space was simply closed with a running barbed V-Lok suture.
The patient was discharged 4 days after surgery without complications. |

 腹腔镜下Whipple手术治疗胰头肿瘤
腹腔镜下Whipple手术治疗胰头肿瘤
 腹腔镜治疗正中弓状韧带综合征(MALS)——
腹腔镜治疗正中弓状韧带综合征(MALS)——
 腹腔镜治疗药物治疗失败后早期小肠梗阻复发
腹腔镜治疗药物治疗失败后早期小肠梗阻复发
 腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴

 发表于 2016-4-4 10:00:16
发表于 2016-4-4 10:00:16
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主