10. Dissection
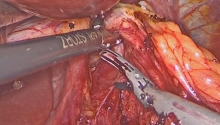
1. Strangulating band
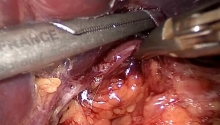
2. Adhesion to the scarred wall
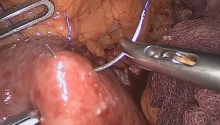
3. Multiple adhesions
Adhesions or bands between the visceral organs and the anterior abdominal wall are freed first. Dissection is performed from the last small bowel loop towards the proximal portion of the small bowel.
Strangulating bands are sectioned with scissors after performing bipolar cauterization.
Freeing of a small bowel loop adhesive to scar tissue can prove to be difficult when the loop is incarcerated in the abdominal wall. During adhesiolysis, the plane of dissection is artificial and situated at a distance from the supposed boundary of the small bowel. Care must be taken to leave some parietal tissue against it. This protects against seromuscular or mucosal leaks in the digestive wall.
Freeing of multiple adhesions between distended intestinal loops remains a very delicate act, because the serosa covering them has often disappeared and the plane of dissection is situated between the two muscle layers. As it is sometimes difficult to find, the exposure must be excellent and the operative act requires precision.
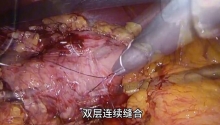
In the presence of an obvious adhesive obstructive site (flattened loops of small bowel coming after the obstruction and distended loops of small bowel coming before it), it is not necessary to perform total adhesiolysis of the small bowel, but only of the obstructive site. On the contrary, with a clinical picture indicating multiple adhesions without clear boundaries between flattened and distended loops of small bowel, the entire jejunoileum must be freed (frequent conversion). |

 腹腔镜治疗正中弓状韧带综合征(MALS)——
腹腔镜治疗正中弓状韧带综合征(MALS)——
 腹腔镜治疗药物治疗失败后早期小肠梗阻复发
腹腔镜治疗药物治疗失败后早期小肠梗阻复发
 腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
 腹腔镜下全结肠切除术联合末端回肠造口术治
腹腔镜下全结肠切除术联合末端回肠造口术治

 楼主
楼主



 显身卡
显身卡