13. Division/sigmoid
Once it is freed, the sigmoid colon is resected. Total resection of the sigmoid colon, including the rectosigmoid junction, is performed. Cephalad, the proximal division is performed on a portion of the colon that is supple and without any diverticula.
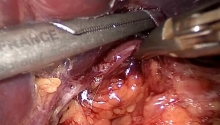
After division of the mesorectum, the distal division of the sigmoid colon is performed below the rectosigmoid junction. The junction is identified on the anterior surface of the rectum by the coalescence of the anterior tenia, and posteriorly by the first collateral branch of the superior rectal vessels.
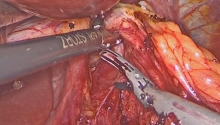
Division of the rectum is performed using a mechanical linear stapling device, which can divide and staple without opening the digestive tract. The stapler is introduced through trocar C into the right iliac fossa. We prefer using staples for thick tissues (green cartridges, 4.8 mm), applied perpendicular to the digestive tract. The use of reticulating staplers may be useful.
• Proximal division
The proximal division should be performed in a non-inflamed area on a perfectly healthy and supple portion of the colon. It includes division of the mesocolon, followed by division of the colon. The division of the mesocolon is always performed in the abdominal cavity. The colon may be divided outside of the abdominal cavity, after it is exteriorized.
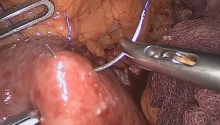
Division is performed with a high-frequency hemostasis device, ultrasonic dissectors, monopolar scissors or linear staplers. The marginal arteries are preserved up to the area of transection.
Whether the colon is divided intracorporeally or extracorporeally, it is important to perform this mesocolic division first because it prevents the mesentery from tearing (during the extraction of the sigmoid colon).
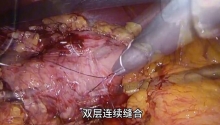
Intracorporeal division is used in surgery for cancer of the sigmoid colon. It is usually performed with a mechanical stapler (blue cartridges) introduced through trocar C into the right iliac fossa. The sigmoid colon is then completely freed.
In sigmoid colectomy for diverticulis, the colon is usually exteriorized before it is divided. The exteriorization is pursued until a healthy portion of colon is reached. The preceding division of the mesocolon facilitates this. |

 腹腔镜治疗正中弓状韧带综合征(MALS)——
腹腔镜治疗正中弓状韧带综合征(MALS)——
 腹腔镜治疗药物治疗失败后早期小肠梗阻复发
腹腔镜治疗药物治疗失败后早期小肠梗阻复发
 腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
腹腔镜全胃切除术联合吲哚菁绿(ICG)淋巴
 腹腔镜下全结肠切除术联合末端回肠造口术治
腹腔镜下全结肠切除术联合末端回肠造口术治

 楼主
楼主








 显身卡
显身卡