First described by Brown in1989, the congenital nasal pyriform aperture stenosis (CNPA) is a uncommon cause of nasal obstruction of the newborn. It is characterized by a narrowing of the nasal cavity (at the beginning of the osseous part) for the excessive growth of the maxilla medial nasal process. It is taken as a minor form of holoprosencephaly, a failure of the development of the prosencephalon and the medial facial structures. Such hypothesis is based on the presence of the solitary maxillary central incisor, which is one of the manifestations of the holoprosencephaly and is present in half of the cases of CNPA. Therefore, despite the CNPA and the presence of the solitary maxillary central incisor can be separate findings, the pituitary hypoplasia and other abnormalities of the central nervous system need to be excluded, preferably with NMR. The CNPA is generally bilateral and manifests upon birth. The CT with parallel cuts of the hard palate is the choice imaging exam. A pyriform aperture is considered to be stenotic when the transversal diameter of each aperture is lower or equal to 3 mm or the total transversal diameter of the pyriform aperture is lower than 8-11mm in a normal newborn. If the patients obtain a good breathing and adequate dietary ingestion with nasal washing, they can be clinically managed, once the symptomatic improvement generally occurs at about 6 months of age. The surgical enlargement of the pyriform aperture is recommended in those patients with breathing and feeding difficulty. The access may be transnasal (technically difficult in the nose of a newborn) or sublabial, with a better viewing and preservation of the nasal mucosa.
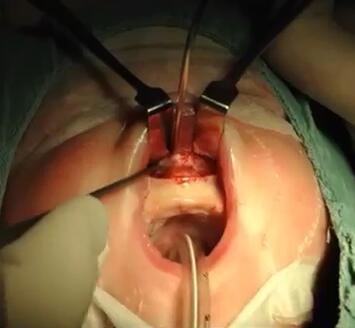
This case is about a newborn with anoxia and seizures postpartum that required immediate intubation. She was transferred to our hospital service with 42 days of life with diagnosis of choanal imperforation. On physical examination we don′t observed oral or nasal external deformities, but we are unable to progression of flexible endoscopes beyond the nasal vestibule bilaterally. A CT scan showed patency in choanal region, but sharp bilateral piriform aperture narrowing (slightly larger than 2 mm transverse diameters of both nostrils) associated with the presence of only one central incisor tooth. After the diagnosis of congenital stenosis of the nostril (ECAP), the child underwent surgery for pyriform aperture enlargement and placement of tracheal tubes number two in each nostril. After 24 hours the Guedel standing since birth were remove and after five days, the nasal tubes too. Unfortunately, despite all the efforts of the team, the child who had never breastfed was unable to suck and swallow milk and therefore the gastric tube could not be removed. Nine days after surgery the patient returned to the originating service for further work stimulation and is recommended to investigate the possibility of central anoxia and complications related to the presence of other potential defects, since the ECAP is considered a minor form of holoprosencephaly, a failure of development of the forebrain and medial facial structures. |

 腹腔镜下胆总管囊肿切除术及高级胆道重建术
腹腔镜下胆总管囊肿切除术及高级胆道重建术
 机器人辅助腹腔镜胆囊次全切除术和胆总管探
机器人辅助腹腔镜胆囊次全切除术和胆总管探
 困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
困难腹腔镜胆囊切除术中的吲哚菁绿荧光胆管
 腹腔镜治疗85岁女性胆石性肠梗阻
腹腔镜治疗85岁女性胆石性肠梗阻

 发表于 2018-1-15 10:59:32
发表于 2018-1-15 10:59:32
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主