Valve-Sparing Aortic Root, Ascending Aorta and Aortic Arch Replacement with Debranching of the Innominate Trunk and Left Common Carotid Artery
Author’s
Paolo Magagna, Stefano Auriemma, Giovanni Domenico Cresce, Tania Francesca Cappellari and Loris Salvador
Department of Cardiovascular Surgery, San Bortolo Hospital, Vicenza - Italy
A 73 year old male presented with an ascending and aortic arch aneurysm with aortic valve insufficiency. No coronaropathy, normal left ventricle function. He had hypertension.
The aortic diameter of the ascending aorta was 57 x 60 mm and the aortic arch diameter was 54 mm on preoperatory Angio-CT scan.
After the sternotomy we incannulate the right axillary artery and the left femoral artery
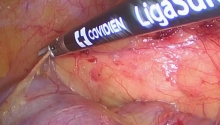
We then prepared the innominate trunk and left carotid artery
Cooling down the patient.
Preparation for the circuit of selective antegrade cerebral perfusion.
Preparation of a number 30 Maquet platinum Hemasheid prothesis
Aortic clamping and retrograde infusion of cold hematic cardioplegia
Removal of the aneurysmal portion of the ascending aorta
Analysis of the valve leaflets
Each commissure is suspended by a U shaped 4.0 polypropylene suture with pledget
The coronary buttons are prepared
The aortic sinus wall is totally removed, a rim of approximally 5 mm of aortic wall is needed to suture the aortic valve to the Valsalva prosthesis
Three sub annular U Sutures, in 3/0 Ethibon non absorbable polyester with pledget, are passed below each commissure.
Preparation of n 30 Vascutek gel weave Valsalva prosthetic with partial removal of the proximal collar: diameter choice of the Valsalva prosthesis is based upon adding 5 mm to the measurement obtained using Hegar’s dilator. In this case the diameter is 25 mm, a 30 mm valve is chosen.
Sub annular stiches are palced on the base of the Valsalva prosthesis
The stitches are tied so as not to stenosis the annulus. This is achieved by tying the same Hegar’s dilator, size 25mm used to choose the prosthesis, inside the annulus.
Resuspension of the commissures at the level of the new sino-tubular junction.
The valve remnants are fixed to the Valsava graft wall corresponding to the new sinus by three continuous 4/0 polypropylene running sutures starting at the nadir of each leaflet towards the top of the commissure. The three sutures are then tied at the top of each commissure.
The coronary ostia are reattached to the skirted portion of the Valsalva graft using a polypropylene 4/0 suture with interposition of a thin layer of Teflon felt.
The proximal anastomosis is performed using the polypropylene 4.0 between the Maquet platinum and Valsava vascular prosthesis, ensuring the correct angle is given to the prosthesis: the branches of the innominate trunk and left common carotid artery must be tilted toward the superior vena cava.
Once the patient's temperature reaches 26 ° C we proceed with circulatory arrest.
Clamping of the Innominate trunk, and perfusion of the right carotid artery through the cannula placed in the right axillary artery (8 ml/kg/min).
Selective antegrade left carotid artery (LCA) perfusion (5 ml/kg/min) monitoring perfusion pressure that is kept above 60 mmHg
The vacuum vent line is inserted through a branch of the prosthesis to keep the operative area bloodless
The vascular prosthesis is resected
The distal anastomosis is performed between the vascular prosthesis and the aortic arch, with a running polypropylene 3-0 suture , with interposition of a thin layer of Teflon felt.
De-airing of the heart and of the vascular prosthesis
Systemic perfusion and myocardial perfusion is reinstated through the femoral artery cannula, while selective antegrade cerebral perfusion is still running through the cannulas place in the left carotid artery and the right axillary artery.
Checking the proximal and the distal anastomoses
Left carotid artery debranching using the n 8 branch of the platinum vascular prosthesis and a continuous polypropylene 5/0 suture: selective antegrade perfusion of the left carotid artery is suspended.
Innominate trunk debranching with the n 10 branch of the platinum vascular prosthesis and a continuous polypropylene 4/0 suture with interposition of a layer of Teflon felt.
Patient rewarming is begun.
The unused branches of the vascular prosthesis are ligated twice and cut and the stump is sutured with a continuous 4/0 polypropylene suture.
Clamping time was 157 minutes, total Cardiopulmonary bypass was 210 minutes; selective antegrade cerebral perfusion of 49 minutes; visceral ischemia was 17 minutes.
Postoperative ventilation time was 5 hours. Time spent in ICU was 23 hours. No major complication occurred.
Postoperative echocardiogram did not show residual aortic insufficiency.
Three month follow-up with angio-CT showed normal patency of the branches of the Innominate trunk and left carotid artery. |

 履带式驼峰
履带式驼峰
 扩展 Kocher,腹腔镜保留幽门 Whipple 的步
扩展 Kocher,腹腔镜保留幽门 Whipple 的步
 机器人辅助简单前列腺切除术_单孔、经膀胱
机器人辅助简单前列腺切除术_单孔、经膀胱
 尾状-先入路腹腔镜右后部分切除术
尾状-先入路腹腔镜右后部分切除术

 发表于 2016-3-19 19:00:03
发表于 2016-3-19 19:00:03
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡 楼主
楼主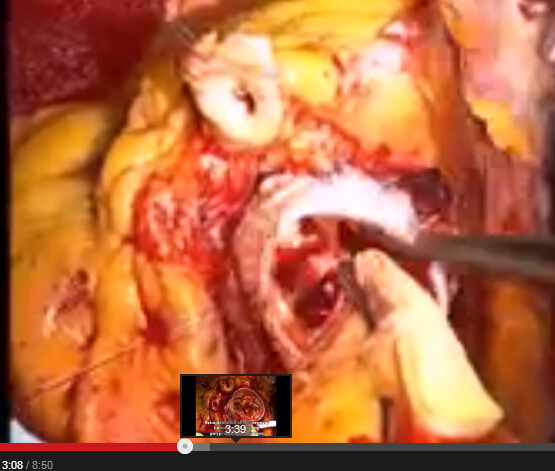
 发表于 2016-3-23 05:31:05
发表于 2016-3-23 05:31:05